Glue ear (Children)
Disclaimer: Disclaimer: This leaflet provides general information and is intended for educational purposes only. It should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare professional for any health concerns or before making any decisions related to your health or treatment.
This leaflet may contain links to external websites or resources (e.g. YouTube) for demonstration purposes; however, these links are provided for information only. Clinicol.co.uk is not affiliated with, does not endorse, and is not responsible for the content, accuracy, or copyright compliance of these external sources. Use of these external links is at your own discretion and risk.
Overview

Glue ear, medically known as Otitis Media with Effusion (OME), is a very common condition where the middle ear fills with a thick, sticky fluid, much like glue. This fluid build-up prevents the eardrum and the tiny bones in the middle ear from vibrating properly, leading to dulled or muffled hearing. It's not an infection, but it can sometimes follow an ear infection.
This condition primarily affects children, especially those under 12 years old, and is incredibly common. Statistics show that around 80% of children will experience glue ear by the age of 10, and many will have had a short episode even before starting primary school. While it can affect one ear, it often occurs in both ears at the same time. The good news is that for most children, glue ear is temporary and clears up on its own, usually within three months to a year, without any specific treatment.
However, the hearing loss caused by glue ear can fluctuate, meaning it might be better on some days and worse on others. If it persists, it can have an impact on a child's development, including their speech, language, behaviour, and social interactions. Understanding glue ear and how to manage it is key to supporting your child through this common childhood experience.
Symptoms and Causes
Understanding the symptoms of glue ear can help you recognise the condition in your child, and knowing the common causes can shed light on why it happens.
Symptoms
The main symptom of glue ear is temporary hearing loss, which can affect one or both ears. Because young children may not be able to tell you directly that their hearing is affected, it's important to look out for other signs. These can include:
- Dulled or Muffled Hearing: Your child might seem to struggle to hear you, especially in noisy environments. They might ask for things to be repeated, speak louder or quieter than usual, or turn up the volume on the television or radio.
- Earache: Some children may experience a mild, dull earache.
- Tinnitus: This is a sensation of ringing, buzzing, or other noises in the ear, which can be distracting.
- Balance Problems: The fluid in the middle ear can sometimes affect balance, leading to clumsiness or difficulties with coordination.
- Speech and Language Delays: If hearing is consistently affected, especially in younger children, it can make it harder for them to hear and learn new words, potentially leading to delays in their speech and language development.
- Behavioural Changes: Children might become more tired, irritable, frustrated, or withdrawn because they are struggling to hear and understand what's happening around them. This can also affect their concentration and progress at school.
- Social Development: Difficulty hearing can make it harder for children to engage in conversations and play with others, potentially impacting their social development.
It's important to remember that these symptoms can fluctuate, meaning they might be more noticeable on some days than others.
Causes
Glue ear occurs when the middle ear, the air-filled space behind the eardrum, fills with fluid. This usually happens because the Eustachian tube isn't working properly. The Eustachian tube is a narrow tube that connects the middle ear to the back of the throat. Its job is to ventilate the middle ear, drain fluid, and keep the air pressure equal on both sides of the eardrum.
In children, the Eustachian tube is narrower and more horizontal than in adults, making it more prone to blockages. Common reasons for the Eustachian tube to become blocked or malfunction include:
- Colds, Flu, and Allergies: These conditions can cause swelling and mucus production in the nose and throat, which can block the Eustachian tube.
- Enlarged Adenoids: Adenoids are small lumps of tissue at the back of the nose, near the opening of the Eustachian tubes. If they become enlarged, they can block the tubes, preventing proper drainage and ventilation of the middle ear.
- Following an Ear Infection: Sometimes, glue ear can develop after an acute ear infection, as fluid can remain in the middle ear even after the infection has cleared.
- Bacteria: Bacteria can travel up the Eustachian tubes, contributing to inflammation and fluid build-up.
- Passive Smoking: Exposure to cigarette smoke can irritate the lining of the Eustachian tube and increase the risk of glue ear.
Certain children are also more susceptible to glue ear, including those with Down's syndrome or a cleft palate, due to differences in their anatomy or immune system.
Diagnosis and Investigations
If you suspect your child has glue ear, the first step is usually to visit your GP. They will be able to assess your child's ears and, if needed, refer them for further tests.
Diagnosis
Your GP will start by asking about your child's symptoms, how long they've been present, and any concerns you have about their hearing or development. This is an important part of understanding the full picture. They will then examine your child's ears using an otoscope, which is a small instrument with a light and a magnifying lens. This allows the doctor to look at the eardrum and check for signs of fluid behind it.
If glue ear is suspected, especially if symptoms have been present for some time, your GP will usually recommend an initial period of 'active monitoring' for about three months. This is because glue ear often clears up on its own. During this time, you'll be given information about the condition, its fluctuating nature, and how it might affect your child. You'll also be advised on communication strategies to help your child hear better at home and at school.
Investigations
If your child's hearing loss persists after the three-month active monitoring period, your GP will refer them to a specialist, such as an audiologist (a hearing specialist) or an ENT (Ear, Nose, and Throat) consultant, for more detailed investigations. These may include:
- Hearing Tests: These are age and developmentally appropriate tests to accurately measure your child's hearing levels. For younger children, this might involve play-based audiometry, where they respond to sounds by performing a simple task. For older children, it might be similar to adult hearing tests.
- Tympanometry: This is a quick and painless test that measures how well your child's eardrum moves. It involves placing a small, soft probe just inside the ear canal. The probe changes the air pressure in the ear and measures the eardrum's response. If there's fluid behind the eardrum, it won't move as freely, which helps confirm the presence of glue ear.
These investigations help the specialists understand the extent of the hearing loss and confirm the diagnosis of glue ear, guiding decisions about the best way forward for your child.
Management and Treatment
The management of glue ear is focused on improving your child's hearing and overall quality of life. Given that many cases resolve naturally, the initial approach is often 'active monitoring'.
Active Monitoring (Watchful Waiting): For suspected or confirmed glue ear with hearing loss, the first step is usually a three-month period of active monitoring. During this time, you and your child's carers (including teachers) will be given detailed information about glue ear, its causes, how it can fluctuate, and its potential impact on hearing, language, behaviour, and social development. You'll also be encouraged to use communication strategies to help your child hear better, such as:
- Getting your child's attention before speaking.
- Speaking clearly and at a normal volume, facing your child.
- Reducing background noise.
- Sitting close to your child during conversations.
- Ensuring teachers are aware of the condition and can adapt classroom seating or communication.
Around half of all glue ear cases clear up on their own within this three-month period. If the glue ear persists and causes significant problems after this time, further options will be considered through shared decision-making with your family.
Treatments if Glue Ear Persists:
- Autoinflation Devices: For children over three years old, devices like the Otovent nasal balloon may be suggested. This involves blowing up a special balloon using one nostril while holding the other nostril closed. This action helps to open the Eustachian tube and can sometimes help to clear the fluid. Another method is swallowing with nostrils closed.
- Temporary Hearing Aids: If the hearing loss is significant and impacting your child's daily life, temporary hearing aids can be a very effective solution. These devices amplify sound, helping your child to hear more clearly. They are particularly useful for children with conditions like Down's syndrome or cleft palate, who may be more prone to persistent glue ear.
- Surgical Intervention: If glue ear continues to cause problems despite other measures, surgical options may be discussed. These include:
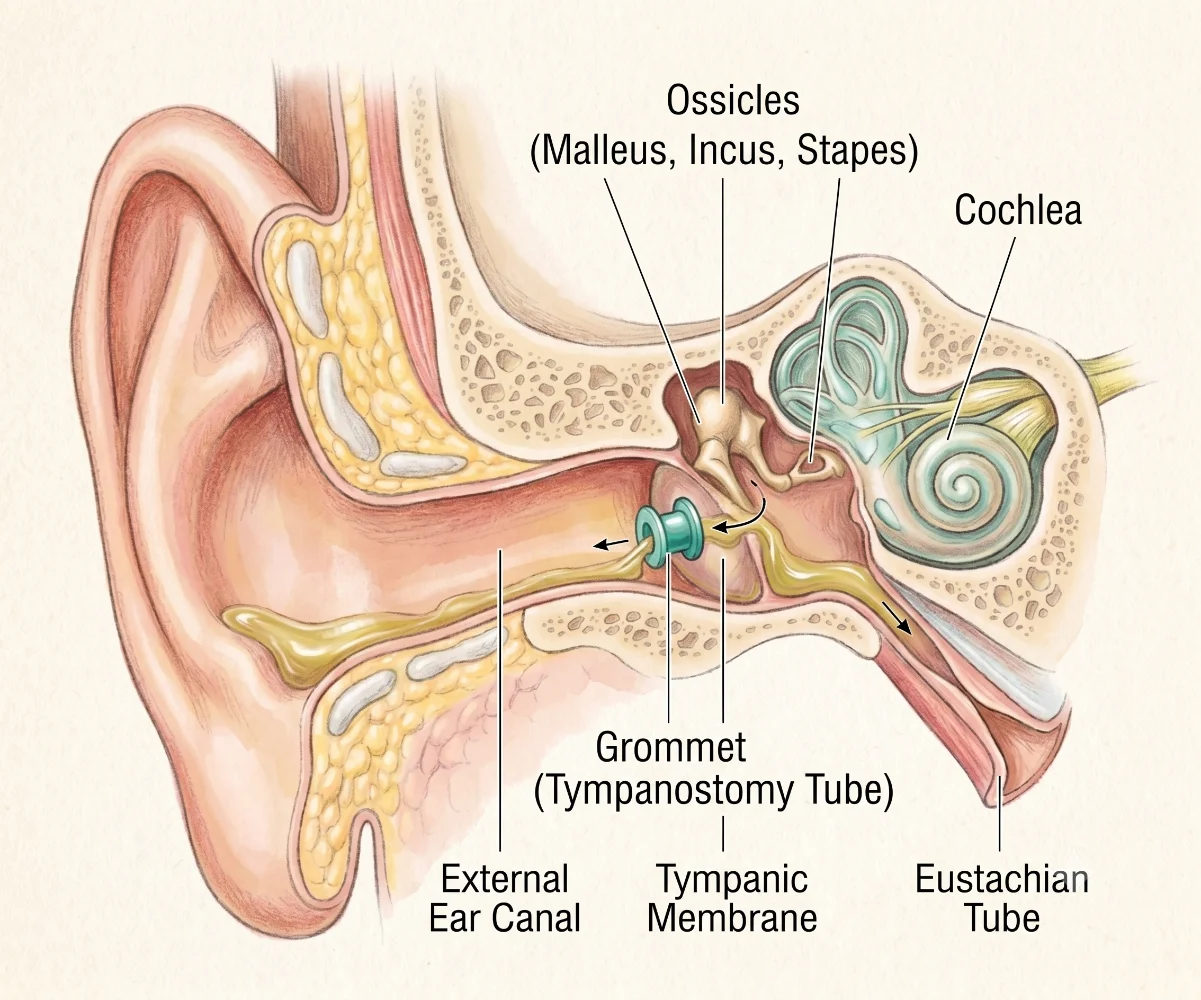
- Grommet Insertion: This is a common procedure where tiny ventilation tubes, called grommets, are inserted into the eardrum. These small tubes act like a tiny drain, allowing air into the middle ear and helping any fluid to drain away. Grommets typically stay in place for 6 to 18 months before falling out naturally as the eardrum heals.
- Adenoidectomy: In some cases, especially if enlarged adenoids are thought to be contributing to the problem, the surgeon might recommend removing the adenoids (adenoidectomy) at the same time as grommet insertion. Removing the adenoids can help improve the function of the Eustachian tubes.
What is NOT Recommended: It's important to know that certain treatments are generally not recommended for glue ear because they have not been shown to be effective. These include antibiotics (unless there's an active ear infection), oral or nasal steroids, antihistamines, leukotriene receptor antagonists, mucolytics, proton pump inhibitors, or decongestants.
If your child has ear discharge (otorrhoea) after grommet insertion, non-ototoxic topical antibiotic drops (drops that won't harm the inner ear) might be considered, but this would be an off-label use and discussed carefully with your specialist.
For adults experiencing glue ear, a referral to an ENT specialist is always advised to investigate the underlying cause.
Prevention
While it's not always possible to completely prevent glue ear, especially given how common it is in children, there are some general approaches that might help reduce the risk or impact:
- Minimising Exposure to Colds and Flu: Since glue ear often follows common colds and flu, encouraging good hand hygiene and avoiding close contact with sick individuals can help reduce the frequency of these infections.
- Avoiding Passive Smoking: Exposure to cigarette smoke is known to be a risk factor for glue ear. Ensuring your child is in a smoke-free environment can help protect their ear health.
- Managing Allergies: If your child has known allergies, working with your doctor to manage these effectively might help reduce inflammation in the nasal passages and Eustachian tubes.
- Early Identification and Intervention: Being aware of the signs and symptoms of glue ear and seeking medical advice promptly can lead to earlier identification. This allows for active monitoring and, if necessary, timely intervention, which can help prevent potential long-term impacts on development.
It's important to remember that glue ear is a very common part of childhood, and even with preventative measures, many children will still experience it. The focus should be on monitoring and appropriate management.
Outlook / Prognosis
The outlook for children with glue ear is generally very positive. For the vast majority, the fluid in the middle ear clears up naturally without any specific treatment. About half of all cases resolve within three months, and most will clear within a year. While glue ear can sometimes recur, it typically becomes less common as children get older, usually resolving completely by around eight years of age.
However, if glue ear persists and causes significant hearing loss that is left unaddressed, there can be potential long-term consequences. These may include delays in speech and language development, difficulties with learning and school progress, and challenges with social interaction and behaviour. This is why active monitoring and, if necessary, intervention are so important.
If your child receives treatment, such as grommet insertion, the aim is to restore normal hearing quickly. Grommets typically fall out on their own as the eardrum heals, and hearing usually returns to normal. Even if grommets are needed multiple times, or if hearing aids are used, children can thrive and develop well with the right support.
The key to a positive outcome is early identification of the condition and its impact, followed by appropriate monitoring and management tailored to your child's individual needs. With careful attention from parents, carers, and healthcare professionals, children with glue ear can achieve excellent long-term hearing and developmental outcomes.
Need Expert Advice?
Book a consultation with Mr Ahmad Hariri to discuss your symptoms and treatment options.
Book a Consultation