Sudden Sensorineural Hearing Loss
Disclaimer: Disclaimer: This leaflet provides general information and is intended for educational purposes only. It should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare professional for any health concerns or before making any decisions related to your health or treatment.
This leaflet may contain links to external websites or resources (e.g. YouTube) for demonstration purposes; however, these links are provided for information only. Clinicol.co.uk is not affiliated with, does not endorse, and is not responsible for the content, accuracy, or copyright compliance of these external sources. Use of these external links is at your own discretion and risk.
Overview
Sudden Sensorineural Hearing Loss (SSNHL), often called sudden deafness, is a rapid loss of hearing that occurs over a period of 72 hours or less. It typically affects only one ear (unilateral). This type of hearing loss originates in the inner ear (cochlea) or the auditory nerve connecting the ear to the brain.
SSNHL is considered an ENT emergency. If you experience a sudden drop in your hearing, it is crucial to seek medical attention immediately, ideally from an Accident & Emergency (A&E) department or an urgent ENT clinic. Prompt diagnosis and treatment offer the best chance of hearing recovery, as the sooner treatment is started, ideally within the first few days, the better the potential outcome.
Symptoms and Causes
Symptoms:
- Rapid Hearing Loss: The most common symptom is a sudden, noticeable decrease in hearing in one ear. Patients might describe it as waking up with deafness, hearing a 'pop' followed by hearing loss, or difficulty using the phone on the affected side.
- Tinnitus: A ringing, buzzing, hissing, or roaring sound in the affected ear.
- Aural Fullness: A feeling of pressure or blockage in the ear.
- Vertigo/Dizziness: A spinning sensation or unsteadiness may accompany the hearing loss in about 30-40% of cases.
Causes: In about 90% of cases, the exact cause of SSNHL is unknown (idiopathic). However, several potential causes and associated factors have been identified, including:
- Viral Infections: Viruses (like those causing mumps, measles, herpes simplex, or upper respiratory infections) can sometimes inflame the inner ear or auditory nerve.
- Vascular Issues: Disruption of blood supply to the inner ear (like a small stroke in the inner ear arteries).
- Autoimmune Diseases: Conditions where the body's immune system mistakenly attacks the inner ear structures.
- Trauma: Head injury or sudden exposure to extremely loud noise.
- Neurological Conditions: Such as Multiple Sclerosis (MS).
- Ototoxic Medications: Certain drugs known to potentially damage the inner ear (less common as a cause of sudden loss).
- Tumours: Very rarely, a benign tumour on the hearing or balance nerve (acoustic neuroma) can present with sudden hearing loss.
Diagnosis and Investigations
Diagnosing SSNHL involves confirming the type and severity of hearing loss and trying to identify any underlying cause.

- Medical History: Your doctor will ask detailed questions about how and when the hearing loss started, any associated symptoms (dizziness, tinnitus), your general health, medications, and any recent illnesses or injuries.
- Physical Examination: An examination of your ears, nose, and throat, including looking at your eardrum (otoscopy).
- Hearing Test (Pure Tone Audiogram - PTA): This is the most crucial test. It measures your hearing thresholds across different frequencies (pitches) in both ears and confirms whether the hearing loss is sensorineural (inner ear/nerve related) and how severe it is. This test needs to be performed urgently.
- Tympanometry: A test to check the function of your middle ear and eardrum.
- Blood Tests: May be requested if an underlying infection or autoimmune condition is suspected.
- MRI Scan: An MRI scan of the brain and inner ears is often recommended, usually after initial treatment. While most scans are normal, it helps rule out rare underlying causes like an acoustic neuroma or other neurological issues.
Management and Treatment
Time is critical in treating SSNHL. Treatment should ideally start as soon as possible after the onset of symptoms, preferably within the first few days, and certainly within the first two weeks for the best effect. Benefit decreases significantly after this time, although treatment might still be considered up to 4-6 weeks in some cases based on clinical judgement.
It's important to know that some hearing recovery can happen on its own, without any treatment (spontaneous recovery). Studies suggest this might occur in about 32% to 65% of cases, often within the first two weeks. However, treatment aims to significantly improve these chances and the degree of recovery.
Oral Corticosteroids: The most common initial treatment is a course of high-dose steroid tablets, usually taken for 1-2 weeks. A common dose and steroid used is often Oral prednisolone 1mg/kg/day (max 60mg/day) for 7 days followed by a tapering dose reduced by 10mg every day:
Day | Day 1-7 | Day 8 | Day 9 | Day 10 | Day 11 | Day 12 | Day 13 |
Prednisolone Dose | 60mg | 50mg | 40mg | 30mg | 20mg | 10mg | STOP |
- Steroids work by reducing inflammation and swelling, which may help the inner ear or nerve recover. While studies vary and the exact benefit is debated, oral steroids are commonly offered as they may increase the chance of meaningful hearing recovery. Some research suggests recovery rates could improve from around 32-35% without treatment to about 50-60% with steroids, particularly noted in older studies.
- Your doctor will discuss potential side effects (e.g., mood changes, sleep disturbance, increased appetite, stomach irritation, temporary rise in blood sugar) and check if they are suitable for you.
Intratympanic Steroid Injections (Salvage Therapy): If your hearing does not improve significantly with oral steroids, or if you cannot take oral steroids due to other health conditions, your consultant may offer intratympanic steroid injections.
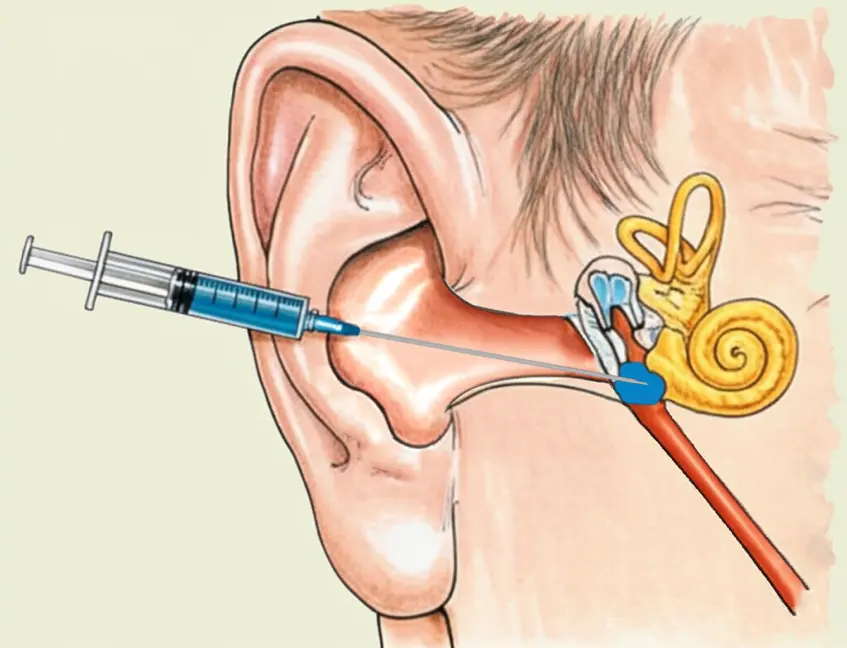
- What is it? This procedure involves injecting a steroid solution directly through the eardrum into the middle ear space. The steroid can then be absorbed into the inner ear.
- How is it done? It is usually performed in an outpatient clinic. Your eardrum is numbed with a local anaesthetic, and then a fine needle is used to inject the steroid. The procedure is relatively quick. There isn't one standard schedule for injections; common approaches involve several injections given over 1-4 weeks (e.g., weekly for 3 weeks, three times in one week, or other protocols depending on local practice and response). Your consultant will discuss the specific plan.
- Why is it done? It delivers a high concentration of steroid directly to the target area with fewer body-wide side effects compared to oral steroids. It is often used as a "salvage" treatment when initial oral therapy hasn't worked well. Studies suggest that around 40% to 56% of patients who haven't recovered sufficiently with oral steroids may gain some hearing improvement (often defined as 10-15 dB gain) with these injections, compared to those who receive no further treatment.
- Risks: Potential side effects include temporary pain, dizziness, a small risk of a persistent hole (perforation) in the eardrum (around 1-2%), infection (rare), or temporary taste disturbance.
Other Treatments: Antiviral medications, vasodilators, or Hyperbaric Oxygen Therapy (HBOT) are sometimes considered, but their effectiveness is less established, and they are not routinely used as standard first-line treatments in the UK.
Prevention
As the cause of SSNHL is often unknown, specific prevention can be difficult. However, general measures to protect your hearing and health may be beneficial:
- Protect your ears from excessive noise exposure (use earplugs or defenders in loud environments).
- Manage underlying health conditions like high blood pressure and diabetes.
- Get recommended vaccinations (e.g., MMR) to prevent viral causes.
- Avoid ototoxic medications where possible (always discuss medication risks with your doctor).
- Seek prompt treatment for any ear infections.
Outlook / Prognosis
The chances of hearing recovery vary significantly from person to person. Factors influencing the prognosis include:
- Severity of the initial hearing loss: More severe (70-90 dB) or profound (>90 dB) hearing loss generally has a lower chance of full recovery compared to mild or moderate loss.
- Pattern of hearing loss: Loss mainly in the high pitches (a 'down-sloping' pattern on the hearing test) or affecting all pitches profoundly ('flat' severe/profound loss) can be harder to recover from than loss mainly in the low pitches ('up-sloping' pattern).
- Presence of vertigo (dizziness) at onset: Often associated with a poorer prognosis.
- Age of the patient: Older patients (e.g., over 60-65 years) sometimes have lower recovery rates than younger patients.
- Time between symptom onset and starting treatment: Delaying treatment beyond the first 7-14 days significantly reduces the chances of recovery.
Some patients experience a full recovery, some have partial recovery, and unfortunately, some have little or no improvement, resulting in permanent hearing loss in the affected ear. Even with prompt and appropriate treatment, recovery is not guaranteed.
If hearing loss persists, management options include:
- Hearing Aids: To amplify sound for the affected ear.
- CROS Aids: For single-sided deafness, these transmit sound from the deaf side to the hearing ear.
- Bone Conduction Hearing Implants: A surgical option for some patients with single-sided deafness.
- Tinnitus Management: Strategies and therapies to help cope with persistent ringing or buzzing.
- Balance Rehabilitation: If dizziness persists.
Your ENT specialist will discuss your specific situation, monitor your hearing with follow-up tests, and advise on the best long-term management plan if needed.
Need Expert Advice?
Book a consultation with Mr Ahmad Hariri to discuss your symptoms and treatment options.
Book a Consultation