Thyroid Nodules
Disclaimer: Disclaimer: This leaflet provides general information and is intended for educational purposes only. It should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare professional for any health concerns or before making any decisions related to your health or treatment.
This leaflet may contain links to external websites or resources (e.g. YouTube) for demonstration purposes; however, these links are provided for information only. Clinicol.co.uk is not affiliated with, does not endorse, and is not responsible for the content, accuracy, or copyright compliance of these external sources. Use of these external links is at your own discretion and risk.
Overview
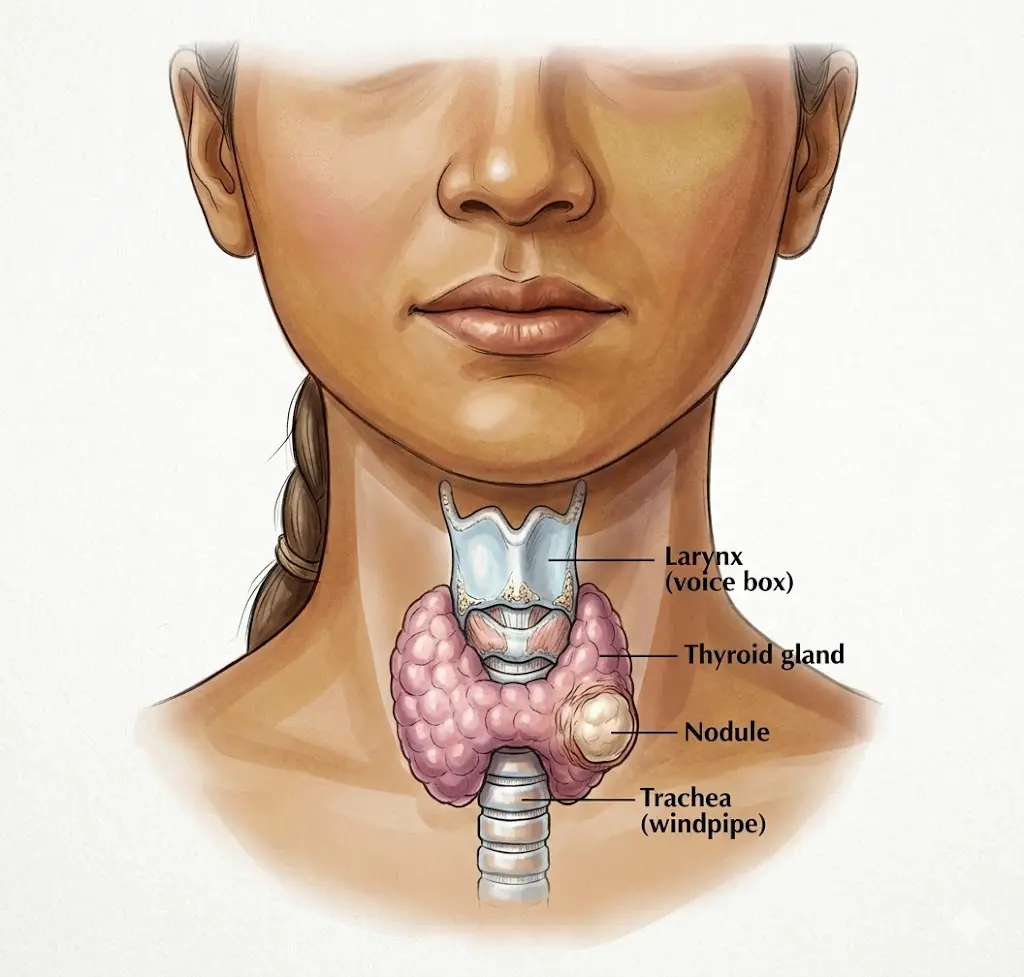
Thyroid nodules are abnormal growths or lumps of cells that form within your thyroid gland. The thyroid gland is a butterfly-shaped organ located at the base of your neck, just below your Adam's apple. It plays a crucial role in producing hormones that regulate many of your body's functions, including metabolism, heart rate, and body temperature.
These nodules are very common. While only about 4 to 7% of adults have thyroid lumps that can be felt by touch (palpable), up to 40 to 50% of people may have nodules detected incidentally (by chance) during an ultrasound scan for another reason. They tend to become more frequent as people get older and are more common in women than in men.
The vast majority of thyroid nodules – over 90 to 95% – are benign, meaning they are non-cancerous. However, a small percentage (around 5%) can be cancerous. Thyroid cancer accounts for about 1% of all cancers. Because of this, the main concern when a thyroid nodule is found is to carefully check it to rule out the possibility of cancer.
Thyroid nodules can come in different forms. Some are cystic, meaning they are filled with fluid. Others are colloid nodules, which contain a jelly-like substance. They can also be hyperplastic (an overgrowth of normal thyroid cells) or adenomatous (a type of benign tumour of glandular tissue). Understanding the type of nodule helps your doctor decide on the best course of action.
Symptoms and Causes
Most thyroid nodules do not cause any symptoms and are often discovered during a routine physical examination or an imaging test for another health issue. However, some nodules can lead to noticeable signs or be caused by underlying conditions.
Symptoms
For most people, thyroid nodules are asymptomatic, meaning they don't cause any problems. When symptoms do occur, they are usually related to the size of the nodule or if it's affecting your thyroid hormone levels:
- Difficulty breathing or swallowing: If a nodule grows large enough, it can press on your windpipe (trachea) or food pipe (oesophagus), making it harder to breathe or swallow. You might feel a constant pressure or a 'tickle in the throat'.
- Hoarseness: This is a rare symptom but can be a sign of a more serious issue. Hoarseness (a rough or harsh voice) can occur if a cancerous nodule grows and affects the recurrent laryngeal nerve, which controls your vocal cords.
- Visible lump: You might notice a lump or swelling in your neck, or someone else might point it out to you.
- Symptoms of an overactive thyroid (hyperthyroidism): If the nodule produces too much thyroid hormone, you might experience symptoms like unexplained weight loss, rapid or irregular heartbeat, nervousness, anxiety, tremors, increased sweating, or difficulty sleeping.
- Symptoms of an underactive thyroid (hypothyroidism): If the nodule interferes with normal thyroid function, leading to too little hormone production, you might feel tired, gain weight, feel cold, have dry skin, or experience constipation.
It's important to be aware of certain 'red flag' symptoms that warrant urgent medical attention. These include a nodule that is growing rapidly, unexplained hoarseness, or swollen lymph glands in the neck (cervical lymphadenopathy).
Causes
In many cases, the exact cause of thyroid nodules is unknown. However, several factors are known to contribute to their development or increase the risk of a nodule being cancerous:
- Iodine deficiency: Iodine is essential for thyroid hormone production. A lack of iodine in the diet can lead to the thyroid gland enlarging (a condition called a goitre) and forming nodules. This is less common in the UK due to iodine being added to some foods, but it can still be a factor.
- Autoimmune conditions: These are conditions where your body's immune system mistakenly attacks its own tissues. Examples include:
- Hashimoto's thyroiditis: This condition often leads to an underactive thyroid (hypothyroidism) and can cause the thyroid gland to become lumpy or form nodules.
- Graves' disease: This condition typically causes an overactive thyroid (hyperthyroidism) and can also be associated with thyroid nodules.
- Medications: Certain medications can sometimes contribute to the development of thyroid nodules, such as lithium (used for mood disorders) and amiodarone (used for heart rhythm problems).
- Risk factors for malignancy (cancer): While most nodules are benign, some factors increase the chance of a nodule being cancerous:
- Age: Being under 20 or over 70 years old.
- Radiation exposure: A history of radiation exposure, especially to the head and neck area (e.g., from previous medical treatments).
- Smoking: Smoking is a general risk factor for many cancers, including thyroid cancer.
- Family history: Having a close family member with thyroid cancer or other endocrine tumours (cancers affecting hormone-producing glands).
Diagnosis and Investigations
When a thyroid nodule is suspected or discovered, your doctor will carry out a thorough assessment to determine its nature and whether further investigation is needed. The primary goal is to rule out thyroid cancer.
Diagnosis
The diagnostic process usually begins with a detailed discussion about your medical history and a physical examination:
- Medical history: Your doctor will ask about any symptoms you've experienced, how long you've noticed the nodule, if it has changed in size, and if you have any risk factors for thyroid cancer, such as a family history or previous radiation exposure.
- Physical examination: Your doctor will carefully examine your neck. They will feel your thyroid gland to assess the size, shape, and consistency of any lumps. They will also check for any swollen lymph glands (lymph nodes) in your neck, which could be a sign of cancer spread.
It's important for you to monitor your own neck for any changes. If you notice the lump increasing in size or hardness, new lumps appearing, or if you develop difficulties swallowing, breathing, or hoarseness, you should contact your GP.
Investigations
Following the initial assessment, several tests may be recommended. These are often carried out in a 'One-Stop Clinic' where you can have multiple investigations on the same day.
- Thyroid Function Tests (TFTs): These are blood tests that measure the levels of hormones related to your thyroid gland, specifically Thyroid Stimulating Hormone (TSH), free Thyroxine (fT4), and free Triiodothyronine (fT3). These tests help determine if your thyroid gland is working normally (euthyroid), is underactive (hypothyroid), or overactive (hyperthyroid). It's worth noting that if you have an overactive or underactive thyroid associated with a nodular goitre (an enlarged thyroid gland with nodules), it is generally less likely to be thyroid cancer.
- Ultrasound Scan: This is a key investigation. An ultrasound uses sound waves to create detailed images of your thyroid gland and any nodules. It helps your doctor determine important characteristics of the nodule, such as whether it is solid or fluid-filled (cystic), its exact size, shape, and other features that can indicate the likelihood of cancer. The ultrasound also helps guide further procedures like a biopsy and can check for any enlarged lymph nodes in the neck.
In the UK, doctors often use the British Thyroid Association (BTA) U-classification system (U1 to U5) to assess the risk of malignancy (cancer) based on the ultrasound features:

- U1: Normal thyroid.
- U2: Benign (non-cancerous) features. These nodules generally do not require a biopsy unless they are very large (4 centimetres or more) or if there's a strong clinical suspicion of cancer.
- U3: Indeterminate features. The risk of cancer is uncertain, and a biopsy is usually recommended.
- U4: Suspicious features. There is a higher suspicion of cancer, and a biopsy is strongly recommended.
- U5: Malignant (cancerous) features. There is a very high likelihood of cancer, and a biopsy is essential.
- Fine Needle Aspiration Cytology (FNAC) / Biopsy: If the ultrasound scan shows suspicious features (U3 or above), a biopsy is usually performed. This involves using a very thin needle to collect a small sample of cells from the nodule. The procedure is often guided by ultrasound to ensure accuracy. The cells are then sent to a laboratory for examination under a microscope.
The results of the FNAC are also classified, typically using a Thy classification system (Thy1 to Thy5):
It's common to experience some mild discomfort or bruising in the neck after an FNAC, but this is usually temporary. - Thy1: Non-diagnostic (not enough cells for a clear diagnosis).
- Thy2: Benign (non-cancerous).
- Thy3: Follicular lesion of undetermined significance / Atypia of undetermined significance (the cells are abnormal, but it's unclear if they are cancerous).
- Thy4: Suspicious of malignancy (likely cancerous).
- Thy5: Almost definitely cancer.
- Technetium Scan: If you have symptoms of an overactive thyroid (thyrotoxicosis) and initial blood tests for TSH receptor antibodies (which help diagnose Graves' disease) are negative, a technetium scan may be considered. This scan uses a small amount of radioactive material to show how active different parts of your thyroid gland are.
- Urgent Suspected Cancer (USC) Referral: If your doctor has a high suspicion of cancer based on your symptoms, examination, or initial test results, you may be referred urgently to an ENT (Ear, Nose, and Throat) Neck Lump Service. This fast-track referral is typically made for features such as rapid growth of the nodule, unexplained hoarseness, swollen lymph glands in the neck, a history of previous neck radiation, a family history of endocrine tumours, or if you are 16 years old or younger.
Management and Treatment
The management and treatment plan for a thyroid nodule depend entirely on the diagnosis – whether it's benign, suspicious, or cancerous – and whether it's affecting your thyroid hormone levels.
- For Benign Nodules (Thy2, U2):
- Monitoring: If the nodule is confirmed as benign and is not causing any symptoms, often no specific treatment is needed. You may be discharged back to your GP's care with advice to monitor for any future changes. Some clinics may offer periodic follow-up ultrasound scans to check the nodule's size and characteristics over time, while others may discharge you after cancer has been excluded.
- Aspiration: If you have a symptomatic cyst (a fluid-filled nodule) or a predominantly cystic nodule, your doctor may offer to aspirate it. This involves using a needle to drain the fluid, which can relieve pressure and symptoms.
- Ethanol Ablation: If fluid re-accumulates in a cyst after aspiration, ethanol ablation may be considered. This procedure involves injecting alcohol into the cyst to help prevent it from refilling.
- Radiofrequency Ablation: For benign nodules that are causing symptoms (e.g., pressure or cosmetic concerns) but are not cancerous, less invasive treatments like radiofrequency ablation are being explored in ongoing trials. This technique uses heat generated by radio waves to shrink the nodule.
- For Thyroid Dysfunction (Hypothyroidism or Hyperthyroidism):
- Hypothyroidism (Underactive Thyroid): If your thyroid is underactive, you will typically be prescribed levothyroxine, a synthetic thyroid hormone. The dosage will be carefully adjusted to bring your TSH (Thyroid Stimulating Hormone) levels back into the normal range. It's important to maintain the correct dosage, as TSH levels that are too low can carry risks such as atrial fibrillation (an irregular heartbeat) and osteoporosis (weakening of bones). Patients with hypothyroidism associated with a nodular goitre are usually referred to a general endocrine clinic for ongoing management.
- Hyperthyroidism (Overactive Thyroid): If your thyroid is overactive, you may be prescribed medication such as carbimazole. Initial doses can range from 5 to 40mg daily and will be adjusted to control your thyroid hormone levels. Patients with hyperthyroidism associated with a nodular goitre are also typically referred to a general endocrine clinic. The initiation of another thyroid hormone medication called liothyronine is usually restricted to endocrinologists.
- For Suspicious or Malignant Nodules (Thy3-5, U3-5):
- Diagnostic Hemithyroidectomy: If the biopsy results are inconclusive (e.g., Thy3 or Thy4), or if there's a strong suspicion of cancer that cannot be confirmed by FNAC alone, a diagnostic hemithyroidectomy may be recommended. This is a surgical procedure where the nodule and the entire half (lobe) of the thyroid gland containing it are removed. This allows for a comprehensive pathological examination (looking at the tissue under a microscope) to definitively determine if the nodule is cancerous and if it has spread. Further treatment will then be decided based on these detailed pathology results.
- Other Surgical Options: For non-cystic nodules or an enlarged thyroid gland (goitre) causing significant compressive symptoms (pressure on your windpipe or food pipe), surgery may be an option to remove part or all of the thyroid gland.
- Radioactive Iodine Ablation: In some cases, for non-cystic nodules or goitres causing compressive symptoms, radioactive iodine ablation might be considered. This treatment uses radioactive iodine to destroy overactive thyroid cells or reduce the size of the gland.
- Percutaneous Thermal Ablation: Similar to radiofrequency ablation, other percutaneous thermal ablation techniques (using heat applied through the skin) may be options for non-cystic nodules or goitres causing compressive symptoms.
Prevention
While it's not always possible to prevent thyroid nodules, especially since many causes are unknown, there are some general health practices and awareness points that can be helpful:
- Maintain a balanced diet: In the UK, iodine deficiency is less common due to iodine being present in various foods, including dairy products, seafood, and iodised salt. A balanced diet generally provides sufficient iodine. However, if you have concerns about your iodine intake, discuss this with your doctor or a dietitian.
- Avoid unnecessary radiation exposure: If you have a history of radiation exposure to the head and neck, or if you are undergoing medical imaging, discuss the necessity of radiation-based scans with your doctor.
- Stop smoking: Smoking is a known risk factor for many cancers, including thyroid cancer. Quitting smoking can significantly improve your overall health and reduce your risk.
- Be aware of family history: If you have a close family member with thyroid cancer or other endocrine tumours, make sure to inform your doctor. This information helps them assess your risk and guide any necessary monitoring.
- Regular self-checks: Periodically checking your neck for any new lumps, swellings, or changes in existing nodules can help with early detection. If you notice anything unusual, contact your GP.
- Prompt medical attention: If you experience any concerning symptoms such as rapid growth of a lump, unexplained hoarseness, or difficulty swallowing or breathing, seek medical advice promptly. Early detection and diagnosis are crucial for effective management.
Outlook / Prognosis
The long-term outlook for individuals with thyroid nodules is generally very positive, especially given that the vast majority are benign. Your prognosis (the likely course of your condition) largely depends on the specific diagnosis and how it is managed.
- For Benign Nodules:
If your nodule is confirmed as benign (non-cancerous), the outlook is excellent. Many benign nodules do not require any active treatment beyond initial diagnosis and reassurance. You will typically be discharged back to your GP's care. It is important to remain vigilant and continue to monitor your neck for any future changes, such as the nodule increasing in size or hardness, the appearance of new lumps, or the development of symptoms like difficulty swallowing, breathing, or hoarseness. If any of these changes occur, you should contact your GP for further assessment.
For benign nodules that cause symptoms (e.g., large size causing pressure), treatments like aspiration or ablation can effectively reduce their size and relieve discomfort, allowing you to live comfortably without ongoing issues. - For Malignant Nodules (Thyroid Cancer):
If a thyroid nodule is found to be cancerous, it's natural to feel concerned. However, the prognosis for most types of thyroid cancer is generally very good, particularly when detected early. Untreated cancerous nodules can grow into surrounding structures in the neck, potentially affecting the vocal cord nerve (which could cause hoarseness) or pressing on the windpipe. This is why early and accurate diagnosis is so important.
Following treatment for thyroid cancer, which often involves surgery to remove part or all of the thyroid gland, you may require lifelong thyroid hormone replacement therapy with levothyroxine. This medication helps to maintain normal body functions and can also play a role in preventing the cancer from returning. Regular follow-up appointments, including blood tests and imaging, will be necessary to monitor your recovery and check for any signs of recurrence or new nodules.
Overall, whether your thyroid nodule is benign or malignant, effective management and appropriate follow-up care mean that most people with thyroid nodules can expect to live full and healthy lives.
Need Expert Advice?
Book a consultation with Mr Ahmad Hariri to discuss your symptoms and treatment options.
Book a Consultation