Reviewed by Mr Ahmad A. Hariri - Consultant ENT, Head & Neck and Thyroid Surgeon.
Disclaimer: Disclaimer: This leaflet provides general information and is intended for educational purposes only. It should not be used as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare professional for any health concerns or before making any decisions related to your health or treatment.
This leaflet may contain links to external websites or resources (e.g. YouTube) for demonstration purposes; however, these links are provided for information only. Clinicol.co.uk is not affiliated with, does not endorse, and is not responsible for the content, accuracy, or copyright compliance of these external sources. Use of these external links is at your own discretion and risk.
Contents
This leaflet provides general information about having a partial thyroidectomy (removal of part of the thyroid gland). This includes procedures like hemithyroidectomy (thyroid lobectomy), isthmusectomy, and subtotal thyroidectomy.
What is the Thyroid Gland and What Does It Do?
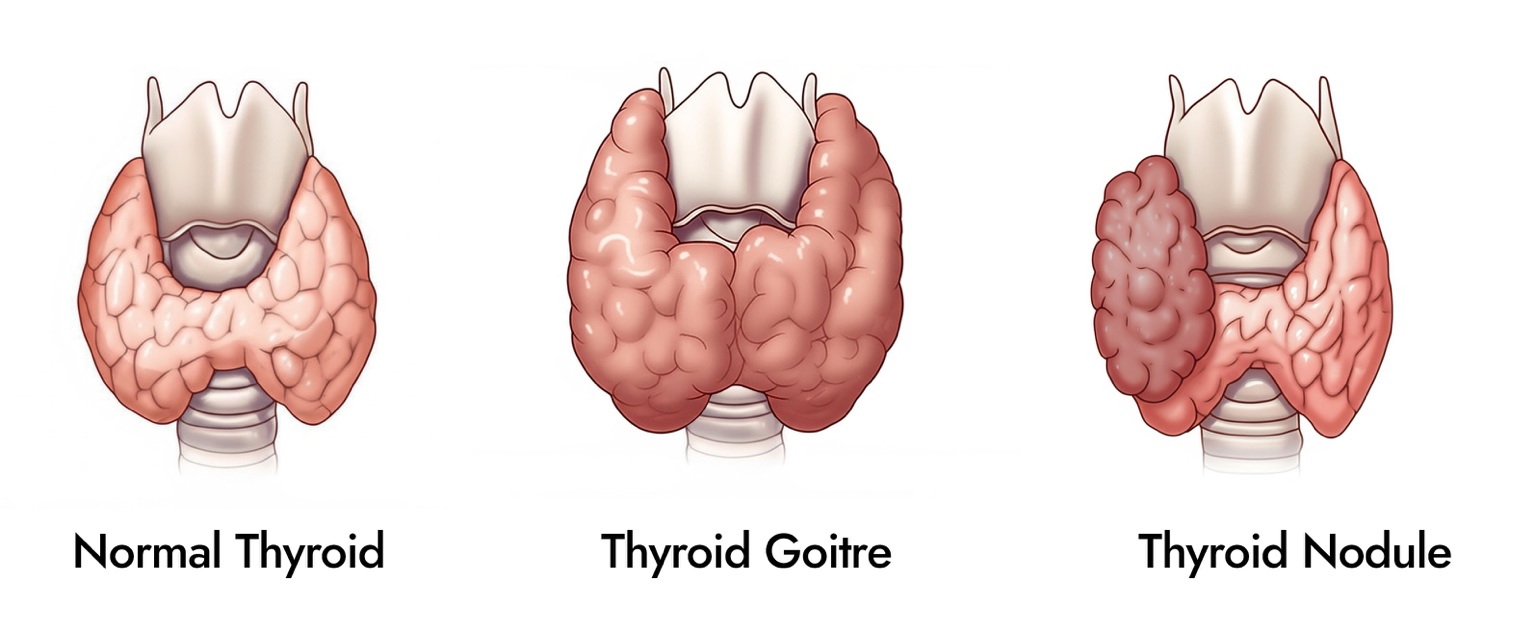
The thyroid gland is a small, butterfly-shaped endocrine gland located in the lower part of the front of your neck, just below your Adam's apple (or where it would be). It has two lobes, one on each side of your windpipe (trachea), which are connected by a narrow bridge of tissue called the isthmus.
The main job of the thyroid gland is to produce thyroid hormones, primarily thyroxine (T4) and triiodothyronine (T3). These hormones are released into your bloodstream and travel to all parts of your body. They play a crucial role in regulating your body's metabolism – the speed at which your body cells and functions work. If your thyroid produces too much hormone (hyperthyroidism or thyrotoxicosis), your body's processes speed up. If it produces too little hormone (hypothyroidism), your body's processes slow down.
What is a Partial Thyroidectomy?
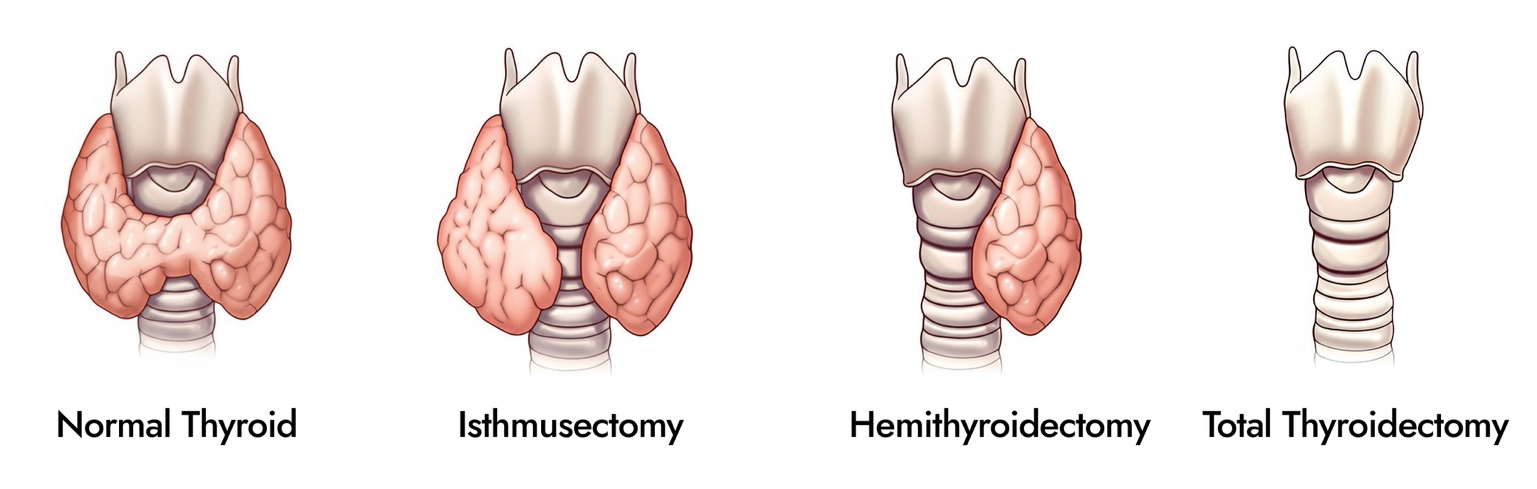
A partial thyroidectomy is a surgical operation to remove only a portion of your thyroid gland. The specific type of partial thyroidectomy depends on how much and which part of the gland is removed:
Hemithyroidectomy or Thyroid Lobectomy: This is the most common type of partial thyroidectomy and involves removing one entire lobe (half) of the thyroid gland.
Isthmusectomy: This procedure involves removing only the isthmus, the central part of the thyroid gland that connects the two lobes. This is often done for small nodules located within the isthmus.
Subtotal Thyroidectomy: This involves removing most of the thyroid gland but leaving a small amount of thyroid tissue behind, usually on one or both sides. This procedure is rarely carried out now.
Your surgeon will explain which type of partial thyroidectomy is recommended for you and why.
Why Might I Need a Partial Thyroidectomy?
Surgery to remove part of the thyroid gland may be recommended for several reasons:
Diagnostic Purposes: If you have a thyroid nodule or swelling in one lobe that is suspicious (e.g., based on ultrasound or an inconclusive needle biopsy), a hemithyroidectomy may be performed to remove the nodule and surrounding lobe for detailed examination by a pathologist to get a definitive diagnosis.
Benign (Non-Cancerous) Nodules or Cysts: If a benign nodule or cyst is large, causing symptoms (like pressure, difficulty swallowing or breathing), or is cosmetically concerning, removing the affected part of the thyroid can resolve these issues.
Overactive (Toxic) Nodule: If a single nodule in your thyroid is overproducing thyroid hormone, removing the lobe containing that nodule (hemithyroidectomy) can cure the hyperthyroidism.
Small, Localized Thyroid Cancer: In certain cases of small, early-stage thyroid cancer confined to one lobe, a hemithyroidectomy may be sufficient treatment.
Goitre (Enlarged Thyroid Gland) Affecting One Lobe or Isthmus: If only a portion of your thyroid is enlarged and causing compressive symptoms or is unsightly.
Your surgeon will discuss the specific reasons for recommending a partial thyroidectomy in your individual case.
What Happens Before Surgery?
Before your operation, several steps will be taken:
Outpatient Consultation: You will meet with your surgeon to discuss the operation in detail. This will include why the surgery is needed, which part of the thyroid will be removed, the procedure itself, potential risks, and what to expect during recovery. You may also meet a clinical nurse specialist for further information and support. This is an important time to ask any questions you have.
Informed Consent: Your surgeon will ensure you understand the operation and will ask for your informed consent to proceed.
Pre-operative Assessment: Usually one to two weeks before your surgery, you will attend a pre-operative assessment clinic. A specialist nurse will:
Review your general health and medical history.
Ask about any medications you are currently taking (please bring a list).
Arrange any necessary tests, such as:
Routine blood tests (including thyroid function and possibly calcium levels as a baseline).
You may also be seen by an anaesthetist or a doctor if needed.
Voice Assessment: Your surgeon will check your vocal cord function before surgery to ensure that they are functioning normally.
Medication Adjustments: You will be advised if you need to stop any medications before surgery, such as aspirin, anti-inflammatory drugs, or blood thinners (e.g., Warfarin).
Smoking: If you smoke, it is strongly advised to stop or significantly reduce smoking well before your surgery, and for at least 24 hours before your anaesthetic, to aid healing and reduce anaesthetic risks.
Fasting: You will receive specific instructions about when to stop eating and drinking before your operation.
What Happens During Surgery?
The operation is performed under a general anaesthetic, so you will be asleep throughout.
Incision: The surgeon will make a cut (incision) in a natural skin crease in the lower part of your neck.
Procedure: The surgeon will carefully identify and protect important structures in your neck on the side being operated on. These include:
The recurrent laryngeal nerve, which controls your voice box on that side.
The parathyroid glands on that side, which control calcium levels. Efforts are made to preserve these glands and their blood supply.
Removal of Thyroid Tissue: The planned portion of your thyroid gland (one lobe for a hemithyroidectomy, the isthmus for an isthmusectomy, or most of the gland for a subtotal thyroidectomy) will be carefully removed. The remaining part of your thyroid gland (if any) is left in place.
Wound Closure: The incision is usually closed with dissolvable sutures (stitches) underneath the skin. The skin surface may then be sealed with surgical glue or sometimes fine strips of sticky tape (Steristrips).
Drain: A small plastic tube (drain) may occasionally be placed in the wound to remove any excess fluid. This is usually removed a day or so later.
Duration: The operation typically takes 1 to 2 hours, but this can vary.
What Happens After Surgery?
After your operation, you will be moved to a recovery area and then to the ward.
Observation: Nurses will monitor you, checking your blood pressure, pulse, oxygen levels, and your wound.
Pain Relief: You may have some soreness in your neck. Pain relief medication will be provided to keep you comfortable.
Position: You will likely be encouraged to sit fairly upright to help reduce swelling.
Voice: Your voice might sound a little hoarse or weak. This is common and usually temporary.
Calcium Levels:
After a hemithyroidectomy or isthmusectomy, problems with low calcium are very rare because the parathyroid glands on the unoperated side are undisturbed and continue to function normally. Blood calcium levels may still be checked as a precaution.
After a subtotal thyroidectomy, there is a higher risk of temporary (or rarely, permanent) low calcium, similar to a total thyroidectomy, depending on how much thyroid tissue and how many parathyroid glands are affected. If this applies to you, your calcium levels will be monitored more closely.
Report any tingling in your lips, fingers, or toes, or muscle cramps to your nurse or doctor immediately.
Eating and Drinking: You can usually start drinking fluids soon after the operation and eat as soon as you feel able.
Drain Removal: If a drain was used, it will be removed when drainage is minimal.
Mobilisation: You will be encouraged to get out of bed and walk around with assistance, usually starting the day after surgery.
Hospital Stay: For an uncomplicated hemithyroidectomy or isthmusectomy, you may stay in hospital for 1 night. A subtotal thyroidectomy might require a slightly longer stay.
Discharge: Before going home, you'll receive instructions on wound care, any necessary medications, and details for your follow-up appointment.
What are the Potential Risks and Complications?
All operations carry some risk. Your surgeon will discuss these with you. For a partial thyroidectomy, potential risks include:
General Anaesthetic Risks: These are rare and will be discussed by your anaesthetist.
Bleeding (Haematoma): A collection of blood under the skin. This is uncommon and usually occurs soon after surgery. If significant, it might require a return to theatre.
Wound Infection: Rare, usually treatable with antibiotics.
Scar: You will have a scar, usually in a neck crease, which typically fades well over time.
Abnormal Scarring (Keloid or Hypertrophic): Rare, but some individuals may develop thicker scars.
Numbness/Tightness around the scar: Common initially and usually improves.
Seroma: A collection of clear fluid under the scar, usually resolves on its own.
Voice Change (Dysphonia):
Temporary Hoarseness/Weakness: Can occur due to bruising of the recurrent laryngeal nerve on the side of surgery, swelling, or the breathing tube. Usually recovers within days to weeks.
Permanent Recurrent Laryngeal Nerve Injury (on the operated side): Occurs in about 1% of cases. Can result in a permanently hoarse or weak voice.
Superior Laryngeal Nerve Injury (on the operated side): Can affect voice projection and pitch. Usually temporary.
Need for Thyroid Hormone Replacement (Hypothyroidism):
After a hemithyroidectomy, the remaining lobe is often able to produce enough thyroid hormone for the body's needs, so many patients (around 70-90%) do not require lifelong thyroid hormone tablets. However, about 10-30% of patients may develop hypothyroidism later and need Levothyroxine.
After an isthmusectomy (if the lobes are healthy), hormone replacement is usually not needed.
After a subtotal thyroidectomy, the need for hormone replacement is more likely, depending on how much functioning thyroid tissue remains.
You will have blood tests after surgery to check the function of your remaining thyroid tissue.
Long-Term Outlook
Thyroid Function: The main long-term consideration after a partial thyroidectomy is the function of your remaining thyroid tissue.
Many patients, especially after a hemithyroidectomy, will maintain normal thyroid function without needing medication.
Regular blood tests (TSH) will be needed to monitor your thyroid hormone levels.
If your remaining thyroid tissue doesn't produce enough hormone (hypothyroidism), you will need to take daily Levothyroxine tablets. Symptoms of hypothyroidism include fatigue, weight gain, dry skin, constipation, and feeling cold. Contact your GP if you develop these.
Calcium Levels: For most partial thyroidectomies (hemithyroidectomy, isthmusectomy), long-term calcium problems are extremely rare. If you had a subtotal thyroidectomy and developed permanent hypoparathyroidism (rare), you would need lifelong calcium and Vitamin D.
Follow-up: You will have follow-up appointments with your surgeon to check your recovery and discuss pathology results. Long-term follow-up will focus on monitoring your thyroid function. If your surgery was for cancer, specific cancer follow-up protocols will apply.
Recovery and Returning to Normal Activities
Wound Care:
If surgical glue was used over dissolvable stitches, you can usually shower the day after surgery. Pat the area dry gently.
If Steristrips were used, try to keep them dry for about a week, or as advised.
Once healed, gentle massage with an unscented moisturising cream can help the scar.
Contact your GP if you see signs of infection (increasing redness, pain, swelling, discharge).
Rest and Activity:
Take it easy for the first 1-2 weeks.
Avoid strenuous activity and heavy lifting until advised by your surgeon (usually 2-4 weeks).
Gentle neck exercises can help with stiffness once healing is underway.
Returning to Work: Usually 1-2 weeks for light duties, longer for more physical jobs.
Driving: When you can comfortably turn your head and are free from significant pain.
Living after a Partial Thyroidectomy
For most people, life after a partial thyroidectomy continues much as before, especially if the remaining thyroid tissue functions normally.
Monitoring: The key aspect is regular monitoring of your thyroid hormone levels through blood tests with your GP.
Awareness: Be aware of the symptoms of an underactive thyroid (hypothyroidism) and report them to your GP if they occur, as you may need to start Levothyroxine.
Medication: If you do need Levothyroxine, it's a simple once-daily tablet.
Support: Patient support organizations like the British Thyroid Foundation can offer information and support.
Most people recover well from a partial thyroidectomy and maintain a good quality of life.
Ready to Take the Next Step?
Book a consultation with Mr Ahmad Hariri to discuss your specific needs and treatment options.